Rett Syndrome





WHAT IS RETT SYNDROME?
Rett syndrome is a neurological disorder that is characterized by normal early growth and development followed by a slowing of development, loss of purposeful use of the hands, slowed brain and head growth, problems with walking, seizures, and intellectual disability. Children often lose ability to speak. Apraxia, the inability to preform motor functions, is the most disabling feature of this syndrome which interferes with every body movement, including eye gaze and speech. About fifty percent of Rett Syndrome sufferers are able to walk.
Children with Rett syndrome often present with Autistic-like symptoms, including toe-walking, wide-based gait, self-stimulating behaviors, irritability, tantrums, incontinence, diminished eye contact, and eating difficulties. They may also have breathing problems such as air swallowing, and apnea (breath holding), and hyperventilation.
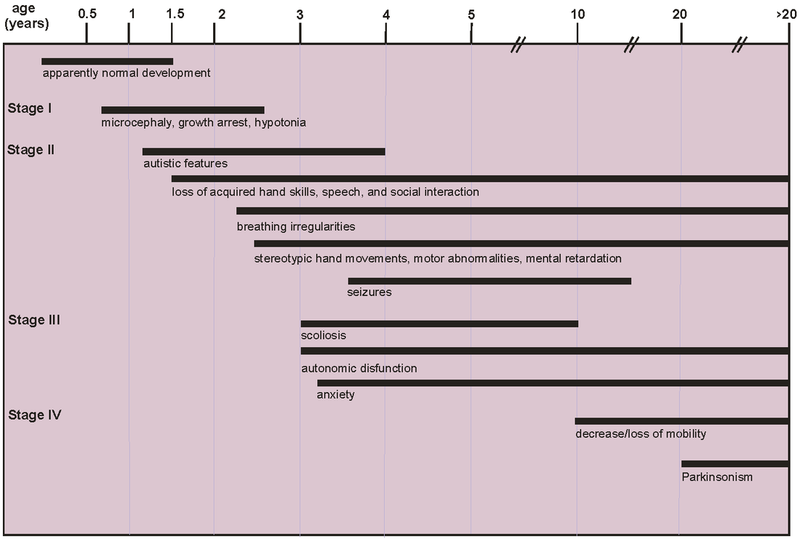
WHAT ARE THE STAGES OF RETT SYNDROME?
- Stage One or "early onset" starts around 6 months to 18 months of age. Children begin to show jerky movements, decreased head growth, decreased interest in toys, and difficulty crawling or sitting up. This stage is often overlooked because changes are subtle. This stage can continue for more than a year.
- Stage Two or the "rapid destructive stage" begins between ages 1 through four, and can last weeks or months. The child loses purposeful hand skills and spoken language skills. Stunted head growth is usually noticed during this stage. Charactersitc hand movements including hand flapping, clapping, and tapping emerge at this stage, as well as breathing issues. Walking and motor movements become difficult. Some children begin to show Autistic-like symptoms of decreased eye contact and loss of social interaction.
- Stage Three or the "plateau" stage begins between ages 2 through 10 and can last for years. Apraxia, motor problems, and seizure are common in this stage. Some behaviors may improve such as increased alertness and decreased irritability. Attention span and communication skills may improve. Individuals can stay in this stage for most of their life.
- Stage Four or the "late motor deterioration stage" can last for years or decades. Notable features include decreased mobility, scoliosis, and muscle rigidity. Individuals who were previously able to walk may lose that ability. Cognition, communication and hand skills generally do not deteriorate in this period. Repetitive movements may decrease and eye contact may increase.
WHO GETS RETT SYNDROME? WHY?
Rett syndrome almost exclusively affects females, but has been found in males as well, on very rare occasions. The syndrome is estimated to effect 10,000 live births per year, and has been recorded in all racial and ethnic groups across the world.
Nearly all cases of Rett Syndrome are caused by a mutation in the MECP2 (pronounced meck-pea-two) gene. The MECP2 gene is found on the X chromosome. The mutation of the gene causes production of irregular proteins in the body, which causes the presenting symptoms of the disorder. Males who have a MECP2 mutation only have one X chromosome (and one Y chromosome) so they lack a second copy of the X chromosome that could compensate for the defective one, and as a result they have no protection from the harmful effects of the genetic defect. Boys with this mutation typically do not show clinical features of Rett syndrome but experience severe problems when they are first born and die shortly after birth.
Although Rett Syndrome is a genetic disorder, less than one percent of cases are inherited or passed from generation to generation. In most cases, the gene mutates randomly and spontaneously. In rare cases, some families with individuals with Rett Syndrome may have another child that has the mutated MECP2 gene but does not show symptoms, and they are referred to as "asymptomatic female carriers".
GET MORE INFORMATION AT NINDS
CLICK ON THE IMAGES BELOW TO EXPLORE FOUNDATIONS, BLOGS, AND ARTICLES ABOUT RETT SYNDROME!

|

|

|

|

|

|
RETT SYNDROME TREATMENT
There is no cure for Rett Syndrome. Treatment is focused on the management of symptoms, and symptoms can vary widely from case to case. Medication is often used to manage seizures, motor difficulties, breathing irregularities, irritability, and to control excessive self-stimulating behavior such as hand flapping and rocking. Occupational therapists can work with children to increase fluency of adaptive and self-care skills like feeding and dressing, as well as other self-direted behaviors like arts & crafts. Physical therapists can work to increase general mobility. Some children require adaptive equipment such as leg braces, back braces, wheelchairs, and splints. Academic, social, and vocational supports may also be required. Not much is known about the life expectancy of an individual with Rett Syndrome, but there are some women in their 40's and 50's that are currently living with the disorder.
Researchers are on the right path to finding a cure for Rett Syndrome. They have isolated the MECP2 gene, and clinical trials have begun using gene therapy to create a normal expression of the proteins generated by that gene. Another option that researchers are exploring is to stop the progression of the disorder by manipulating other genes to compensate for the MECP2 gene. Researchers are also searching for other genes that may be involved with the symptom expression of Rett Syndrome.
HISTORY OF RETT SYNDROME & RETT SYNDROME IN THE DSM-V
Rett Syndrome was discovered by Dr. Andreas Rett, and Austrian physician who first described it in a journal article in 1966. It was not until 1983 when a second article was published about the disorder, penned by Swedish researcher Dr. Bengt Hagberg, that the disorder was generally recognized. The specific gene that causes Rett Syndrome (MECP2) was not isolated until 1999.
The DSM-V has made some drastic changes, and Rett Syndrome is no longer included under Austism Spectrum Disorder (ASD) in the DSM-V. The justification for this exclusion is that ASD is described by specific sets of behaviors, not by biological causes which are present in the diagnosis of Rett. In addition, Autistic-like symptoms are not always present during every stage of the syndrome. The tragedy of removing Rett Syndrome from the ASD blanket of diagnoses is that children with Rett Syndrome will not receive the vast array of services and support that are available to children and families who have an Autism diagnosis.
However, individuals who have Rett Syndrome as well as severe Autistic-like symptoms (which are not necessarily present) can still be described as having ASD, as long as the clinicians uses the specifier "with known genetic or medical condition" to indicate ASD symptoms are related to Rett Syndrome. This way it may still be possible for them to receive Autism services.
|
The document to the right talks about growing up with Rett Syndrome and all the issues that come along with it. Since females with Rett Syndrome can live well into their 40's and 50's, this is a very useful tool for teaching girls what to expect and how to prepare for it... |
|
The video below talks about how Rett Syndrome affects the individual and the family, as well as the outlook for research and treatment of the disorder...
Meet Alicia, and click on her picture to see more stories like hers...

STRATEGIES
Working with students or children with Rett Syndrome can be challenging, but you do not have to do it alone! Here are some helpful options that have worked for others, and may work for you too...
THERAPY OPTIONS
Occupational Therapy
This form of therapy focuses on fine motor skills. Occupational therapists help people participate in things they want and need to do through the therapeutic use of everyday activities (occupations), which includes feeding, grooming, toilet training, and dressing. OT's are focused on adapting the environment to fit the person. The benefits of OT include improved body awareness, coordination, balance, and social interactions through play.
OT's will work with girls with Rett Syndrome on purposeful fine motor function, play skills, and balancing skills by using specific techniques. Such techniques include hand-over-hand assistance with tasks, and engaging them in play. Activities can include banging on drums, clapping along to music, whistling, walking on a balance beam, drawing, push button toys, and blowing bubbles.
link to American Occupational Therapy Association
link to Occupational Therapy Techniques for Children with Autism
Physical Therapy
This form of therapy focuses on gross motor skills. Physical therapists focus on gaining mobility and strengthening the muscles of their clients. PT's are focused on cultivating the skills of the individual to better navigate their environment. The benefits of PT include increased mobility, coordination, strength, play skills (running/jumping) and better muscle tone.
PT's will work with girl with Rett Syndrome on basic motor skills such as sitting, rolling, and standing. They may also do stretches to loosen up muscles and work towards a wider range of motion. Working with kids on jumping, walking, and running are also in a PT's skillset. They may also work on more sophisticated skills such as walking backwards, kicking, and throwing. PT's may use walkers or ballet bars to help children learn how to ultimately walk independently.
link to Physical Therapy as Autism treatment
link to American Physical Therapy Association
ABA Therapy
ABA stands for Applied Behavior Analysis, and it is a behavior and speech modification therapy. This type of therapy is common for children with Autism Spectrum Disorder, and teaches children how to communicate better. ABA identifies measurable problem behaviors, the functions of those behaviors, and creates specified plans to alter that behavior, and then monitors procedures and behavior changes with the applied therapy. Techniques are always being evaluated and changed to get the fastest progression of skills.
ABA values naturalistic implementation in real life situations, when tends to make the more desired behaviors stick. This technique identifies a child's interests and uses that hook to teach important skills for appropriate play behaviors (ex. not throwing or putting toys in mouth) as well as communication behaviors. Verbal Behavior is another ABA technique that teaches children how to communicate with others to get their personal needs met, whether that be through sign language, pointing at cue cards, pressing buttons, or verbally asking questions.
link to National Speech & Language Therapy
link to Massachusetts ABA Center
IN THE CLASSROOM
-do not expect student to keep up with general education curriculum; this will set them up for failure
-create reachable goals for them, regarding what activities/tasks they should complete, and what progress they should make based on their age & intellectual ability
-include occupational skill teaching in classroom (staying calm, play skills)
-assistive technology (picture/memory games
-use ipad to communicate with child, as well as back and forth to parents everyday
-provide an individual aide or separate classroom for one-on-one and small group instruction
-stick with one concept at a time and do not move too quickly with subject matter
-use hand-over-hand techniques for them to complete assignments, artwork, and tasks
-frequent moving/stretching breaks to release energy and anxious feelings
-large grips for writing and drawing utensils
-taking walks (if possible)
-isolated/quiet "cool down" space to get away from overstimulating environments
-singing songs and clapping along to the music
-sensory table play
-visuals & large manipulatives for lessons
-visual schedule and visual cues for transitions
-provide a larger desk with room for a wheelchair to move around and exit safely

|
Click Key Phrases Below for More on Specific Teaching Strategies..
Intellectual disabilities Physical disabilities Behaviors related to Autism Quick Guide for Teaching the Disabled |
The video below shows one family's story, as well as demonstrating various physical therapy and occupational therapy techniques that can have a positive affect on the child's ability to function...

Click on the image to the left to
GET INVOLVED ON FACEBOOK!