
Bipolar Disorder in Children
Welcome to my site on Bipolar Disorder in Children!This site was built based on a long-standing interest I’ve had in Bipolar Disorder. After spending time working with a young Bipolar child, I realized I knew almost nothing about Bipolar beyond the stigma of "uncontrolled anger" and "unpredictable mood swings". I hope this site will help you learn as much as I have to challenge that stigma.
Little research has been done directly on pediatric Bipolar Disorder, but the disorder follows many of the characteristic patterns of adult Bipolar. It is characterized by unusual shifts in mood, between extreme highs called mania and extreme lows of depression, both of which occur outside of the normal “ups and downs” that everyone experiences naturally. Unlike most Bipolar adults, Bipolar children tend to have much more abrupt changes in mood, and cycle more frequently between mania and depression, with less time without symptoms between episodes. Symptoms of mania include inattentiveness, sleeplessness, euphoria and recklessness, and symptoms of depression include anxiety, irritability and thoughts of suicide. Bipolar Disorder is treated with a combination of psychotherapy and intensive medication regimens, which help to dull the extremes of each episode, but also come with various intrusive side effects. Bipolar Disorder significantly affects a child's daily life, and can impact the ability to succeed at school. Educators can be helpful in providing specific, tailored learning accommodations to students, especially in combating the effects of medication programs on learning, and can be a major support in helping these children succeed at school. Explore the site below to learn more about Bipolar Disorder. |
Topics Covered
|
What is Bipolar Disorder?
|
Bipolar disorder is a brain disorder that causes unusual shifts in mood, energy, and activity levels. It can also make it hard to carry out day-to-day tasks, such as going to school or hanging out with friends. Symptoms are different from the normal ups and downs that everyone goes through from time to time.
Doctors diagnose bipolar disorder using guidelines from the Diagnostic and Statistic Manual of Mental Disorders (DSM). To be diagnosed, the symptoms must be a major change from your child's normal mood or behavior. There are four basic types of bipolar disorder:
Symptoms of bipolar disorder most often develop in the late teens or early adult years, but some people have their first symptoms during childhood. Learn more. EtiologyThe exact cause of bipolar disorder is unknown, but several factors seem to be involved in causing and triggering bipolar episodes:
|
|
Symptoms
|
Youth with bipolar disorder experience unusually intense emotional states that occur in distinct periods called "mood episodes." The extreme highs and lows of mood are accompanied by extreme changes in energy, activity, sleep, and behavior. Learn more.
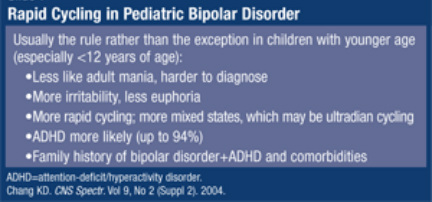
Unlike most adults, children who have pediatric bipolar disorder show abrupt mood swings, periods of hyperactivity followed by lethargy, intense temper tantrums, frustration and defiant behavior. This rapid, severe cycling between moods may produce chronic irritability with few clear periods of peace between episodes. Learn more. Bipolar Disorders in children are severe, highly comorbid, chronic, cyclical, and frequently relapsing biopsychosocial mood disorders of childhood and adolescence. The core symptoms of manic and depressive symptoms can be further exacerbated by the secondary problems of comorbidity; teacher, parent, and sibling stress; sleep disruptions; and time spent out of school. Learn more. 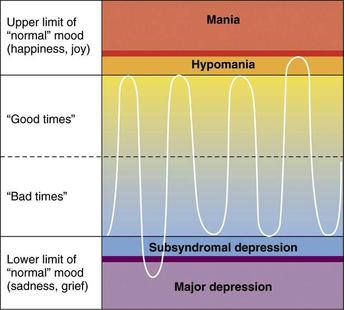
Bipolar episodes occur outside the "normal" limits of mood, on either end of the spectrum.
ManiaBEHAVIORAL CHANGES DURING A MANIC EPISODE
|
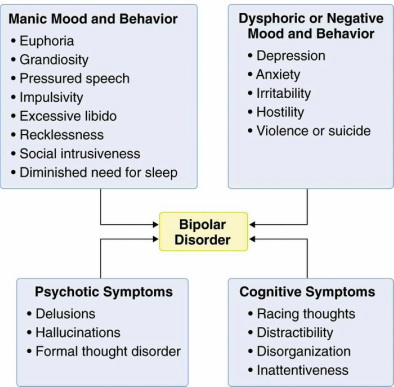
Symptom Categories of Bipolar Disorder
When compared to their adult counterparts, children with Bipolar tend to display more rapid cycling of manic and depressive episodes, with less time in between episodes.
DepressionBEHAVIORAL CHANGES DURING A DEPRESSIVE EPISODE
|
Statistics
There is not much statistical information to date specifically on the prevalence of childhood bipolar disorders. Cases more frequently display onset in later adolescence, with at least half of cases being diagnosed prior to age 25. Though the number of diagnosed bipolar cases in children is rising, there is a lot of controversy over whether these are misdiagnoses of disorders with overlapping symptoms, such as ADHD.
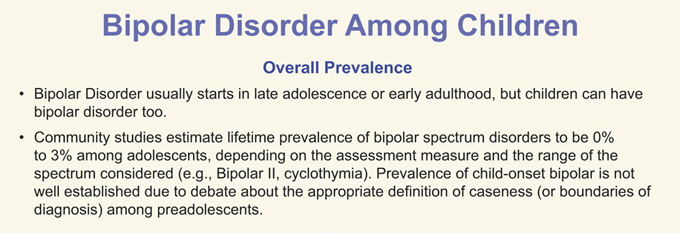
Many individuals who are eventually diagnosed with Bipolar Disorder begin displaying symptoms as young children. There is often a lag in diagnosis because in children the symptoms displayed can also be attributed to disorders such as ADHD or anxiety.
|
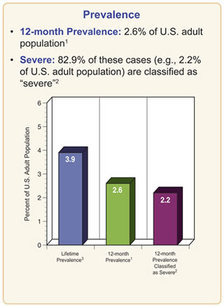
Lifetime Prevalence of Bipolar Disorder among U.S. adults.
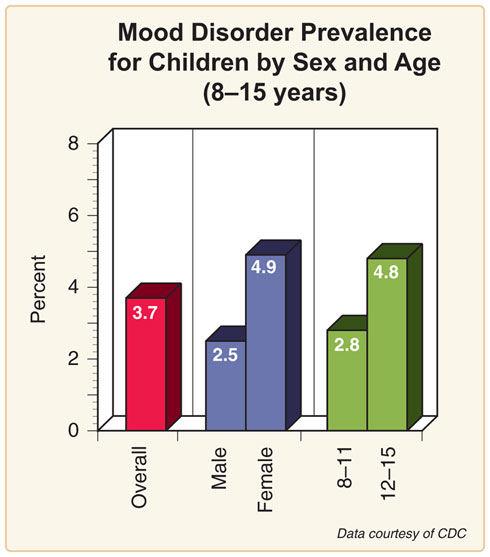
Bipolar Disorder is part of a larger category of Mood Disorders. This chart shows the prevalence and distribution of overall mood disorders in children.
|
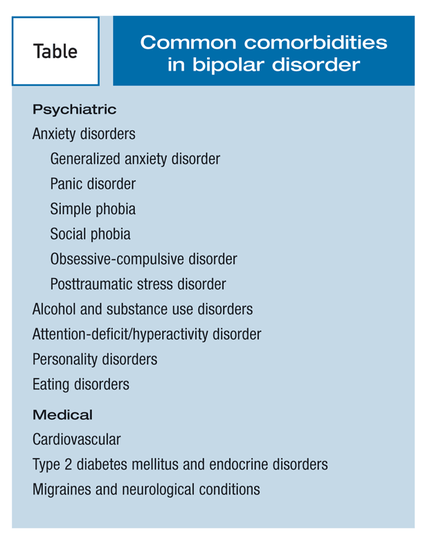
Comorbidity with other Disorders
ADHD
|
It is difficult for clinicians to differentiate mania vs ADHD, and the real problem is comorbidity. ADHD is primarily a disorder of attention, not mood, with an onset before 7 years of age. It tends to be persistent, not episodic. The real problem is that many patients with mania--children and adolescents--tend to also have ADHD.
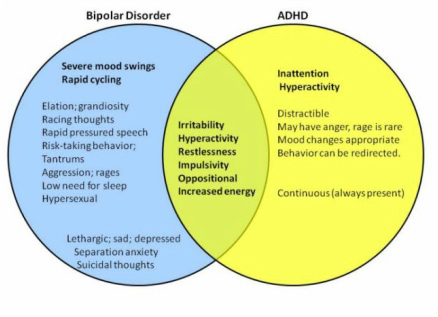
Overlapping symptoms and high rates of comorbidity make diagnosing Bipolar Disorder in children more complicated. This adds to the controversy claiming that Bipolar Disorder is overly diagnosed when mistaking ADHD for a Mood Disorder.
|
|
Treatments
|
There is no cure for Bipolar Disorder. However, through strategic treatment, the symptoms can be managed to lessen the impact on the individual's daily life. Treatments range from psychotherapy to intensive medication programs.
Learn more about treatment options for Bipolar youth. HealthyPlace.com National Institute of Mental Health TherapyCognitive behavioral therapy, which helps young people with bipolar disorder learn to change harmful or negative thought patterns and behaviors.
Family-focused therapy, which includes a child's family members. It helps enhance family coping strategies, such as recognizing new episodes early and helping their child. This therapy also improves communication and problem-solving. Interpersonal and social rhythm therapy, which helps children and teens with bipolar disorder improve their relationships with others and manage their daily routines. Regular daily routines and sleep schedules may help protect against manic episodes. Psychoeducation, which teaches young people with bipolar disorder about the illness and its treatment. This treatment helps people recognize signs of an impending relapse, allowing them time to seek treatment early, before a full-blown episode occurs. Psychoeducation also may be helpful for family members and caregivers. |


|
Medication

|
Mood stabilizers, such as lithium are usually the first choice to treat bipolar disorder. Lithium is approved for the treatment and prevention of manic symptoms in children ages 12 and older. In addition, lithium might act as an antidepressant and help prevent suicidal behavior. However, FDA's approval of lithium was based on treatment studies in adults, not children.
Anticonvulsant medications, originally developed to treat seizures, are also sometimes used as mood stabilizers. They are not approved by the FDA for treating bipolar disorder in children, but your doctor may prescribe one on an "off label" basis. They may be very helpful for difficult-to-treat bipolar episodes. For some children, anticonvulsants may work better than lithium. Examples of anticonvulsant medications include valproic acid or divalproex sodium (Depakote) and lamotrigine (Lamictal). Atypical antipsychotics are sometimes used to treat symptoms of bipolar disorder. Those approved by the FDA to treat youth with bipolar disorder are risperidone (Risperdal), aripiprazole (Abilify), quetiapine (Seroquel), and olanzapine (Zyprexa). Short-term treatment with risperidone can help reduce symptoms of mania or mixed mania in children ages 10 and up. Some research has indicated that risperidone is more effective in treating mania in young children than other medications. Aripiprazole and quetiapine are approved to treat mania symptoms in children 10–17 years old who have bipolar I, while olanzapine is approved for use in children ages 13–17. |
Effects on Learning
Many of the symptoms of Bipolar Disorder, along with those associated with highly common comorbid disorders like ADHD and anxiety, have a tremendous impact on a child's performance in school.
Although research is limited on academic functioning of children with EOBPSD, studies reported that 24% of children with EOBPSD repeated a grade, 13% had learning disabilities, 43% had special education placements, 58% received tutoring, and 30% and 42% had math and reading disabilities, respectively. Learn More.
Although research is limited on academic functioning of children with EOBPSD, studies reported that 24% of children with EOBPSD repeated a grade, 13% had learning disabilities, 43% had special education placements, 58% received tutoring, and 30% and 42% had math and reading disabilities, respectively. Learn More.
|
Common Difficulties in School
Learn More: Massachusetts General Hospital |

|
Medication's Impact on Learning
Many of the medications used to treat children with Bipolar can cause severe side effects that impact every day functioning. Many of these side effects affect a child's attention and physical comfort, and can seriously decrease a child's ability to learn in the classroom.
|
|
|
Learn More: National Institute of Mental Health
Strategies in the Classroom
Symptom: Stress/Irritability
Symptom: Social Difficulties
Symptom: Physical Discomfort from Medication
Read more about these accommodations:
|
Symptom: Impaired Concentration and Focus
Symptom: Sleep Disruption from Medication

|
Resources
This book is a resource for children that helps them understand their diagnosis and offers reassurance and comfort in stressful moments.
|
The Storm in my Brain is a book that addresses how children with mood disorders may feel. It is a great resource for kids, their parents, and educators.
|
This book is on the DBS Alliance's list for best books for parents with Bipolar children.
|
|
For ChildrenKid'sHealth.org - A site that is free of "doctor speak" and is for children and families to learn about all areas of health and growing up.
BPC Children: Kids Page For ParentsDepression and Bipolar Support Alliance - DBSA provides hope, help, support, and education to improve the lives of people who have mood disorders.
The Balanced Mind Parent Network (BMPN), a program of the Depression and Bipolar Support Alliance (DBSA), guides families raising children with mood disorders to the answers, support and stability they seek. BPC Children: Parents Page For EducatorsEducating the Child with Bipolar Disorder - an informative document for educators to understand Bipolar Disorder and to learn methods to accommodate children with Bipolar in the classroom
BPC Children: Teachers Page Educational Issues Facing Children with Bipolar Disorder |