
What is Down Syndrome?
Down syndrome is caused by a chromosomal abnormality in which a person has three copies of chromosome 21 instead of the usual two. It is the most common chromosomal condition. Although people with Down syndrome are often characterized as unintelligent, may are of average intellect, are able to live on their own and even go to college. While people who have Down syndrome have easily recognizable facial features, they are also more prone to many health problems than the rest of the population. Children with Down syndrome are often not as different from their peers as is assumed and the biggest complaint of most parents of children with Down syndrome is that they wish their child was treated like everyone else.
Etiology
|
The word ‘syndrome’ refers to a set of signals and symptoms that tend to occur together and which reflect the presence of a particular disorder or an increased chance of developing a particular disorder. Down syndrome is considered a ‘syndrome’ because it produces a recognizable pattern of differences in different areas of the body.
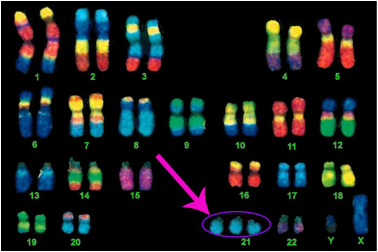
Down syndrome is usually caused by an error in cell division called "nondisjunction." Nondisjunction results in an embryo with three copies of chromosome 21 instead of the usual two. Prior to or at conception, a pair of 21st chromosomes in either |
|
the sperm or the egg fails to separate. As the embryo develops, the extra chromosome is replicated in every cell of the body. This type of Down syndrome, which accounts for 95% of cases, is called trisomy 21.
Learn more about the other two types of Down syndrome, Mosaicsm and Translocation, which account for 5% of Down syndrome cases.
Learn more about the other two types of Down syndrome, Mosaicsm and Translocation, which account for 5% of Down syndrome cases.
Characteristics & Health Issues
|
|
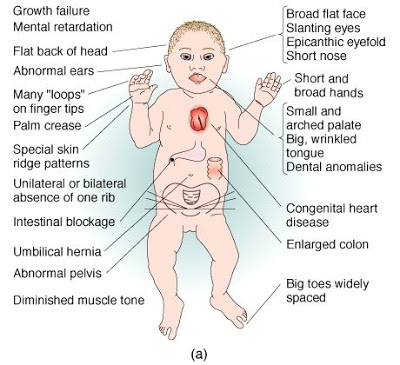
The most common features are upward slanting eyes, a flatter and broader mid-face, a small and flat nose, small ears, short fifth fingers, a wide gap between the first and second toes, low muscle tone, a small mouth with a short roof, and a protruding tongue. The protruding tongue of many people with Down syndrome often causes them articulation problems. The average man is 5’2 while the average woman is more petit at 4’9.
Many people with Down syndrome can have low muscle tone, which plays a large role in physical development early in life. Low muscle tone increases the mobility between joints and directly affects feeding, speech, and gross motor skills, which include rolling over, sitting, standing, and walking. There are also differences between the brains of people with Down syndrome and the brains of people without Down syndrome. The brains of people with Down syndrome have a lack of surface complexity, reduced volume and weight, immature neuronal connections, a smaller cerebellum, immaturity in frontal and temporal lobes, and a hippocampus that is 30-50% smaller in adults. |
People who have Down syndrome are prone to congenital heart conditions at birth, Autism, Celiac disease, eye problems, ear, nose, and throat problems, sleep apnea, hearing loss, blood problems (Leukemia), Alzheimers, thyroid problems, skin problems, delayed motor and speech development.
Learn more about health issues for people with Down Syndrome.
Learn more about health issues for people with Down Syndrome.
Incidence and Prevalance
There are currently about 400,000 people with Down syndrome in the United States and there are approximately 6000 babies born with Down syndrome in the United States every year.
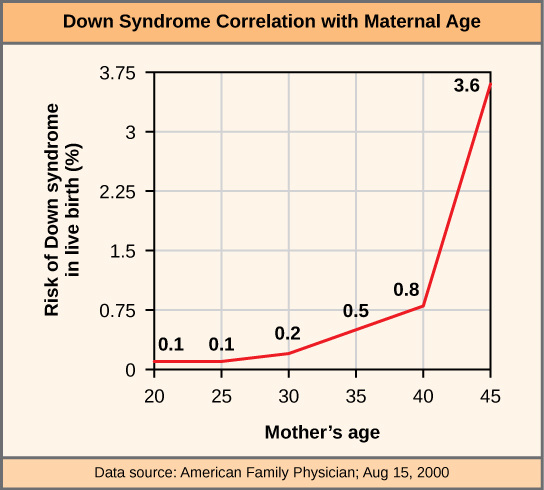
For every girl born with Down syndrome, there are 1.15 boys born with it. In 2016, one out of ever 691 babies born will have Down syndrome, which is an increase from 2010 when one in every 733 was born with Down syndrome. While there are many factors affecting this, it may be cause by more women waiting longer to have children. The chances of a baby having Down syndrome increase with maternal age. At age 35, a woman has a 1 in 350 chance of having a baby with Down syndrome, and at age 40, she has a 1 in 100 chance. By the time a woman is 45, her chances of having a baby with Down syndrome is 1 in 30.
For every girl born with Down syndrome, there are 1.15 boys born with it. In 2016, one out of ever 691 babies born will have Down syndrome, which is an increase from 2010 when one in every 733 was born with Down syndrome. While there are many factors affecting this, it may be cause by more women waiting longer to have children. The chances of a baby having Down syndrome increase with maternal age. At age 35, a woman has a 1 in 350 chance of having a baby with Down syndrome, and at age 40, she has a 1 in 100 chance. By the time a woman is 45, her chances of having a baby with Down syndrome is 1 in 30.
|
|
|
Impact on Learning, Communication and Social Interaction
|
By age five, most children with Down syndrome have a good social understanding, can relate to others, can make friends, can behave in socially appropriate ways, can fit into preschool or kindergarten, are toilet trained, can feed themselves, can run, can kick and catch large balls, use talking as their main for of communication, and are beginning to draw and write.
Most people with Down syndrome have IQs in the mild to moderate range (20-55). They are at par with the general population in recognizing happy, sad, angry and disgusted faces, however, they are deficient at recognizing surprise and fear. People with Down syndrome have problems with short-term memory as well as deficits in auditory and sequential memory. The strength of their visual processing is greater than the strength of their auditory processing. When completing visual and spatial memory tasks, they are usually at or above the ability level of their same age peers. |


|
However, their verbal memory and language skills are usually poorer than their same age peers. On average, children with Down syndrome can remember a list of 3.5 items, which is representative of their lower abilities in verbal short-term memory. Additionally, children with Down syndrome are slower in vocabulary acquisition. However, by their teenage years, vocabulary is considered a strength for people with Down syndrome, meaning that they are able to make up for their later in life start of speech.
People with Down syndrome benefit from continued education and there are not currently enough chances for them to learn the literacy and number skills that are important to everyday life.
People with Down syndrome benefit from continued education and there are not currently enough chances for them to learn the literacy and number skills that are important to everyday life.
Supporting Learning and Increasing Strenths
|
|
The most common forms of early intervention for children with Down syndrome are physical therapy, occupational therapy, and speech and language therapy.
Once they are in school, all children with Down syndrome have an Individualized Education Program (IEP) in order to make sure that they meet all of their educational goals. This provision is part of FAPE in IDEA and applies to students between the ages of three and twenty-one. The IEP team decides what the least restrictive environment (LRE) is for the student. For many students with Down syndrome, the general classroom is the LRE, but this is not true of |
everyone. Some students with Down syndrome are considered too high functioning to be covered by IDEA. These students are protected by section 504 of The Rehabilitation Act of 1973, which prohibits programs receiving federal funding to discriminate against students with disabilities. For example, through section 504, a student with high functioning Down syndrome can be moved to the front of the class if it will be beneficial to his or her learning.
Most teachers are not properly trained to have a student with Down syndrome mainstreamed into their classroom. An even bigger problem is that their expectations for students with Down syndrome are generally lower than they should be. However, if parents, teachers, and professionals give each other proper support and have good communication, inclusion is a beneficial choice for children with Down syndrome. Once they have a student with Down syndrome in their class, most teachers report having a positive experience with them.
Most teachers are not properly trained to have a student with Down syndrome mainstreamed into their classroom. An even bigger problem is that their expectations for students with Down syndrome are generally lower than they should be. However, if parents, teachers, and professionals give each other proper support and have good communication, inclusion is a beneficial choice for children with Down syndrome. Once they have a student with Down syndrome in their class, most teachers report having a positive experience with them.
|
|
|
|
Online Resources
Brighter Tomorrows
Brighter Tomorrows is a web-based resource for parents who have received a diagnosis of Down Syndrome either prenatally or at birth. The site provides answers to common questions, educates about Down Syndrome and shares the stories of other parents with similar situations.
Center for Disease Control and Prevention
The CDC is great for general information about Down Syndrome.
Down Syndrome Pregnancy
This site provides information and support to expectant parents preparing for the birth of a baby with Down Syndrome.
International Mosaic Down Syndrome Association
Offers support and resources to families of and individuals with mosaic Down syndrome through the lifespan.
Medline Plus: Health Topics - Down Syndrome
An overview and list of resources on Down syndrome and prenatal testing from Medline Plus, a service of the US National Library of Medicine and the National Institutes of Health.
National Association for Down Syndrome
NADS is the oldest organization in the country serving individuals with Down syndrome and their families. It was founded in Chicago in 1961 by parents who chose to go against medical advice and raised their children with Down syndrome at home. Their pioneering efforts have made it easier for later generations of individuals with Down syndrome.
National Down Syndrome Society
The mission of the National Down Syndrome Society is to be the national advocate for the value, acceptance and inclusion of people with Down syndrome.
National Society of Genetic Counselors
Find members of NSGC through the Find A Genetic Counselor search function.
Understanding a Down Syndrome Diagnosis
Understanding a Down Syndrome Diagnosis is an accurate, balanced and up-to-date booklet for use when delivering a diagnosis of Down Syndrome. It is available as a free e-book from Lettercase.
Brighter Tomorrows is a web-based resource for parents who have received a diagnosis of Down Syndrome either prenatally or at birth. The site provides answers to common questions, educates about Down Syndrome and shares the stories of other parents with similar situations.
Center for Disease Control and Prevention
The CDC is great for general information about Down Syndrome.
Down Syndrome Pregnancy
This site provides information and support to expectant parents preparing for the birth of a baby with Down Syndrome.
International Mosaic Down Syndrome Association
Offers support and resources to families of and individuals with mosaic Down syndrome through the lifespan.
Medline Plus: Health Topics - Down Syndrome
An overview and list of resources on Down syndrome and prenatal testing from Medline Plus, a service of the US National Library of Medicine and the National Institutes of Health.
National Association for Down Syndrome
NADS is the oldest organization in the country serving individuals with Down syndrome and their families. It was founded in Chicago in 1961 by parents who chose to go against medical advice and raised their children with Down syndrome at home. Their pioneering efforts have made it easier for later generations of individuals with Down syndrome.
National Down Syndrome Society
The mission of the National Down Syndrome Society is to be the national advocate for the value, acceptance and inclusion of people with Down syndrome.
National Society of Genetic Counselors
Find members of NSGC through the Find A Genetic Counselor search function.
Understanding a Down Syndrome Diagnosis
Understanding a Down Syndrome Diagnosis is an accurate, balanced and up-to-date booklet for use when delivering a diagnosis of Down Syndrome. It is available as a free e-book from Lettercase.
Research and Strategy Articles and Books
Cardoso-Martins, C., Peterson, R., Olson, R. & Pennington, B. (March 2009). Component reading skills in Down syndrome. Reading and Writing, 22(3), 277-292.
Coe, D. A., Matson, J. L., Russell, D. W., Slifer, K. J. Capone, G. T., Baglio, C. & Stallings, S. ( April 1999). Behavior problems of children with Down syndrome and life events. Journal of Autism and developmental disorders, 29(2). 149-159.
Education for All Handicapped Children Act, 20 U.S.C. 1400 (1975).
Freeman, S. F. N., Alkin, M. C. & Kasari, C. L. (May/June 1999). Satisfaction and desire for change in educational placement for children with Down syndrome: perceptions of parents. Remedial and Special Education, 20(3), 143-151.
Heward, W. L. (2009). Exceptional children: an introduction to special education (9th ed.). Upper Saddle River: Pearson.
Individuals with Disabilities Education Improvement Act of 2004, 20 U.S.C. 1415 (2004).
Jarrold, C., Baddeley, A. D., & Phillips, C. E. (June 2002). Verbal short-term memory in Down syndrome: a problem of memory, audition, or speech? Journal of Speech, Language, and Hearing Research, 45(3), 531-544.
Olsen, C. L., Cross, P. K., Gensburg & L. J. (August 2003). Down syndrome: interaction between culture, demography, and biology in determining the prevalence of a genetic trait. Human Biology, 75(4), 503-520.
Perez-Padilla, R., Fernandez, R. Garcia-Sancho, C., Franco-Marina, F., Aburto, O., Lopez-Gatell & Bojorquez, L. (August 2010). Pandemic (H1N1) 2009 virus and Down syndrome patients. Emerging Infectious Diseases, 16(8), 1312-1317.
Section 504 of the Rehabilitation Act of 1973, 29 U.S.C. 794 (1973).
Skallerup, S. (Ed.). (2008). Babies with Down syndrome: a new parents guide (3rd ed.). Bethesda: Woodbine House.
Strauss, D. & Eyman, R. K. (May 1996). Mortality of people with mental retardation in California with and without Down syndrome, 1986-1991. American Journal on Mental Retardation, 100, 643-653.
Wishart, J. G. & Pitcairn, T. K. (November 2000). Recognition of identity and expression in faces by children with Down syndrome. American Journal on Mental Retardation, 105(6), 466-479.
Wishart, J. G. (Summer 1998). Development in children with Down syndrome, facts findings, the future. International Journal of Disability, Development, and Education, 45(3), 343-363.
Wolpert, G. (1996). The education challenges inclusion study. New York, NY: National Down Syndrome Society.
Coe, D. A., Matson, J. L., Russell, D. W., Slifer, K. J. Capone, G. T., Baglio, C. & Stallings, S. ( April 1999). Behavior problems of children with Down syndrome and life events. Journal of Autism and developmental disorders, 29(2). 149-159.
Education for All Handicapped Children Act, 20 U.S.C. 1400 (1975).
Freeman, S. F. N., Alkin, M. C. & Kasari, C. L. (May/June 1999). Satisfaction and desire for change in educational placement for children with Down syndrome: perceptions of parents. Remedial and Special Education, 20(3), 143-151.
Heward, W. L. (2009). Exceptional children: an introduction to special education (9th ed.). Upper Saddle River: Pearson.
Individuals with Disabilities Education Improvement Act of 2004, 20 U.S.C. 1415 (2004).
Jarrold, C., Baddeley, A. D., & Phillips, C. E. (June 2002). Verbal short-term memory in Down syndrome: a problem of memory, audition, or speech? Journal of Speech, Language, and Hearing Research, 45(3), 531-544.
Olsen, C. L., Cross, P. K., Gensburg & L. J. (August 2003). Down syndrome: interaction between culture, demography, and biology in determining the prevalence of a genetic trait. Human Biology, 75(4), 503-520.
Perez-Padilla, R., Fernandez, R. Garcia-Sancho, C., Franco-Marina, F., Aburto, O., Lopez-Gatell & Bojorquez, L. (August 2010). Pandemic (H1N1) 2009 virus and Down syndrome patients. Emerging Infectious Diseases, 16(8), 1312-1317.
Section 504 of the Rehabilitation Act of 1973, 29 U.S.C. 794 (1973).
Skallerup, S. (Ed.). (2008). Babies with Down syndrome: a new parents guide (3rd ed.). Bethesda: Woodbine House.
Strauss, D. & Eyman, R. K. (May 1996). Mortality of people with mental retardation in California with and without Down syndrome, 1986-1991. American Journal on Mental Retardation, 100, 643-653.
Wishart, J. G. & Pitcairn, T. K. (November 2000). Recognition of identity and expression in faces by children with Down syndrome. American Journal on Mental Retardation, 105(6), 466-479.
Wishart, J. G. (Summer 1998). Development in children with Down syndrome, facts findings, the future. International Journal of Disability, Development, and Education, 45(3), 343-363.
Wolpert, G. (1996). The education challenges inclusion study. New York, NY: National Down Syndrome Society.