Autism Spectrum Disorder Awareness
The purpose of this website is to raise awareness to children on the autism spectrum. In this site you will find information about Autism Spectrum Disorder, including the latest DSM classification; explanations of autism for adults and children; signs of autism in children; what children with autism want you to know; myths about autism; and how teachers can implement classroom strategies to accommadate children with autism.
“It takes a village to raise a child. It takes a child with autism to raise the consciousness of the village,” Coach Elaine Hall
“It takes a village to raise a child. It takes a child with autism to raise the consciousness of the village,” Coach Elaine Hall
Latest DSM Classification of Autism Spectrum Disorder

|
Autism spectrum disorder (ASD) is the name for a group of developmental disorders. ASD includes a wide range, “a spectrum,” of symptoms, skills, and levels of disability.
People with ASD often have these characteristics:
|
|
|
|
Signs of Autism Spectrum Disorder
Autism spectrum disorders affect three different areas of a child's life:
Sometimes, a child's development is delayed from birth. Some children seem to develop normally before they suddenly lose social or language skills. Others show normal development until they have enough language to demonstrate unusual thoughts and preoccupations.
In some children, a loss of language is the major impairment. In others, unusual behaviors (like spending hours lining up toys) seem to be the dominant factors.
Parents are usually the first to notice something is wrong. But a diagnosis of autism is often delayed. Parents or a physician may downplay earlysigns of autism, suggesting the symptoms are "just a phase" or a sign of a minor delay in development. Children with a possible autism spectrum disorder, though, should be evaluated by a professional team with experience in diagnosing autism.
Until recently, the types of ASD have been determined by guidelines in the diagnostic manual (DSM - IV) of the American Psychiatric Association. According to the CDC, the three main types of ASD are:
The new diagnostic manual has made some major changes in this list of disorders. It's unclear, though, how these changes will affect the way health professionals define exactly what is an autistic spectrum disorder.
Autism spectrum disorders affect three different areas of a child's life:
- Social interaction
- Communication -- both verbal and nonverbal
- Behaviors and interests
Sometimes, a child's development is delayed from birth. Some children seem to develop normally before they suddenly lose social or language skills. Others show normal development until they have enough language to demonstrate unusual thoughts and preoccupations.
In some children, a loss of language is the major impairment. In others, unusual behaviors (like spending hours lining up toys) seem to be the dominant factors.
Parents are usually the first to notice something is wrong. But a diagnosis of autism is often delayed. Parents or a physician may downplay earlysigns of autism, suggesting the symptoms are "just a phase" or a sign of a minor delay in development. Children with a possible autism spectrum disorder, though, should be evaluated by a professional team with experience in diagnosing autism.
Until recently, the types of ASD have been determined by guidelines in the diagnostic manual (DSM - IV) of the American Psychiatric Association. According to the CDC, the three main types of ASD are:
- Asperger's syndrome
- Pervasive developmental disorder, not otherwise specified (PDD-NOS)
- Autistic disorder
The new diagnostic manual has made some major changes in this list of disorders. It's unclear, though, how these changes will affect the way health professionals define exactly what is an autistic spectrum disorder.
|
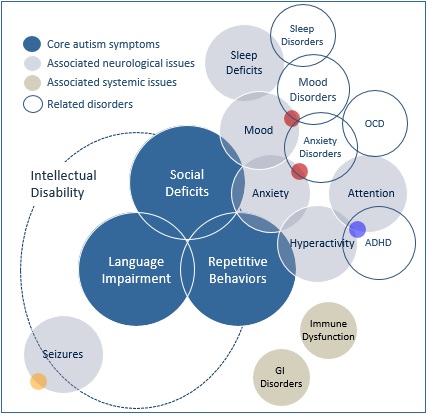
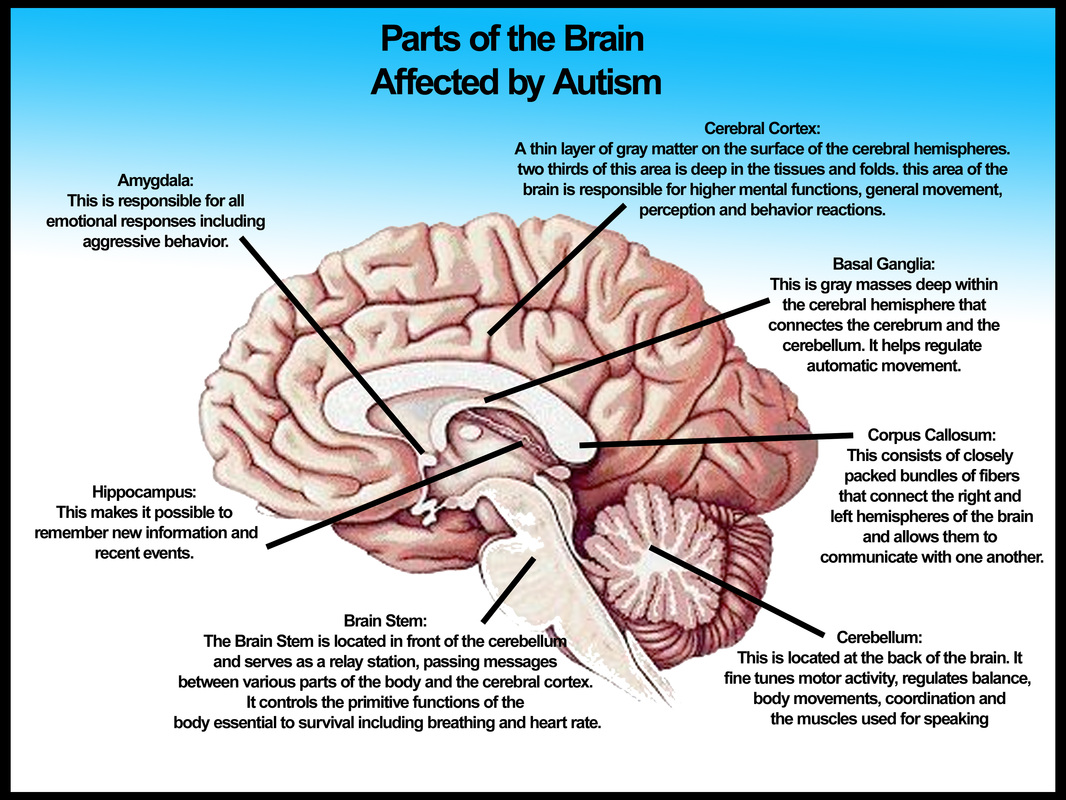
Symptons associated with autism
|
What Children with Autism want you to know
10. I am a child. My autism is part of who I am, not all of who I am. Are you just one thing, or are you a person with thoughts, feelings, preferences, ideas, talents, and dreams? Are you fat (overweight), myopic (wear glasses) or klutzy (uncoordinated)? Those may be things that I see first when I meet you, but you’re more than just that, aren’t you?
As an adult, you have control over how you define yourself. If you want to single out one characteristic, you can make that known. As a child, I am still unfolding. Neither you nor I yet know what I may be capable of. If you think of me as just one thing, you run the danger of setting up an expectation that may be too low. And if I get a sense that you don’t think I “can do it,” my natural response will be, why try?
9. My senses are out of sync.This means that ordinary sights, sounds, smells, tastes, and touches that you may not even notice can be downright painful for me. My environment often feels hostile. I may appear withdrawn or belligerent or mean to you, but I’m just trying to defend myself. Here’s why a simple trip to the grocery store may be agonizing for me.
My hearing may be hyperacute. Dozens of people jabber at once. The loudspeaker booms today’s special. Music blares from the sound system. Registers beep and cough, a coffee grinder chugs. The meat cutter screeches, babies wail, carts creak, the fluorescent lighting hums. My brain can’t filter all the input and I’m in overload!
My sense of smell may be highly sensitive. The fish at the meat counter isn’t quite fresh, the guy standing next to us hasn’t showered today, the deli is handing out sausage samples, the baby in line ahead of us has a poopy diaper, they’re mopping up pickles on aisle three with ammonia. I feel like throwing up.
And there’s so much hitting my eyes! The fluorescent light is not only too bright, it flickers. The space seems to be moving; the pulsating light bounces off everything and distorts what I am seeing. There are too many items for me to be able to focus (my brain may compensate with tunnel vision), swirling fans on the ceiling, so many bodies in constant motion. All this affects how I feel just standing there, and now I can’t even tell where my body is in space.
8. Distinguish between won’t (I choose not to) and can’t (I am not able to).It isn’t that I don’t listen to instructions. It’s that I can’t understand you. When you call to me from across the room, I hear, Jordan.” Instead, come over to me, get my attention, and speak in plain words: “Jordan, put your book in your desk. It’s time to go to lunch.” This tells me what you want me to do and what is going to happen next. Now it’s much easier for me to comply.
7. I’m a concrete thinker. I interpret language literally.You confuse me by saying, “Hold your horses, cowboy!” when what you mean is, “Stop running.” Don’t tell me something is “a piece of cake” when there’s no dessert in sight and what you mean is, “This will be easy for you to do.” When you say, “It’s pouring cats and dogs,” I see pets coming out of a pitcher. Tell me, “It’s raining hard.”
Idioms, puns, nuances, inferences, metaphors, allusions, and sarcasm are lost on me.
6. Listen to all the ways I’m trying to communicate.It’s hard for me to tell you what I need when I don’t have a way to describe my feelings. I may be hungry, frustrated, frightened, or confused but right now I can’t find those words. Be alert for body language, withdrawal, agitation or other signs that tell you something is wrong. They’re there.
Or, you may hear me compensate for not having all the words I need by sounding like a little professor or movie star, rattling off words or whole scripts well beyond my developmental age. I’ve memorized these messages from the world around me because I know I am expected to speak when spoken to. They may come from books, television, or the speech of other people. Grown-ups call it echolalia. I may not understand the context or the terminology I’m using. I just know that it gets me off the hook for coming up with a reply.
5. Picture this! I’m visually oriented.Show me how to do something rather than just telling me. And be prepared to show me many times. Lots of patient practice helps me learn.
Visual supports help me move through my day. They relieve me of the stress of having to remember what comes next, make for smooth transition between activities, and help me manage my time and meet your expectations.
I need to see something to learn it, because spoken words are like steam to me; they evaporate in an instant, before I have a chance to make sense of them. I don’t have instant-processing skills. Instructions and information presented to me visually can stay in front of me for as long as I need, and will be just the same when I come back to them later. Without this, I live the constant frustration of knowing that I’m missing big blocks of information and expectations, and am helpless to do anything about it.
4. Focus and build on what I can do rather than what I can’t do. Like any person, I can’t learn in an environment where I’m constantly made to feel that I’m not good enough and that I need fixing. I avoid trying anything new when I’m sure all I’ll get is criticism, no matter how “constructive” you think you’re being. Look for my strengths and you will find them. There is more than one right way to do most things.
3. Help me with social interactions.It may look like I don’t want to play with the other kids on the playground, but it may be that I simply do not know how to start a conversation or join their play. Teach me how to play with others. Encourage other children to invite me to play along. I might be delighted to be included.
I do best in structured play activities that have a clear beginning and end. I don’t know how to read facial expressions, body language, or the emotions of others. Coach me. If I laugh when Emily falls off the slide, it’s not that I think it’s funny. It’s that I don’t know what to say. Talk to me about Emily’s feelings and teach me to ask, “Are you okay?”
2. Identify what triggers my meltdowns. Meltdowns and blow-ups are more horrid for me than they are for you. They occur because one or more of my senses has gone into overload, or because I’ve been pushed past the limit of my social abilities. If you can figure out why my meltdowns occur, they can be prevented. Keep a log noting times, settings, people, and activities. A pattern may emerge.
Remember that everything I do is a form of communication. It tells you, when my words cannot, how I’m reacting to what is happening around me. My behavior may have a physical cause. Food allergies and sensitivities sleep problems and gastrointestinal problems can all affect my behavior. Look for signs, because I may not be able to tell you about these things.
1. Love me unconditionally.Throw away thoughts like, “If you would just—” and “Why can’t you—?” You didn’t fulfill every expectation your parents had for you and you wouldn’t like being constantly reminded of it. I didn’t choose to have autism. Remember that it’s happening to me, not you. Without your support, my chances of growing up to be successful and independent are slim. With your support and guidance, the possibilities are broader than you might think.
Three words we both need to live by: Patience. Patience. Patience.
View my autism as a different ability rather than a disability. Look past what you may see as limitations and see my strengths. I may not be good at eye contact or conversation, but have you noticed that I don’t lie, cheat at games, or pass judgment on other people?
I rely on you. All that I might become won’t happen without you as my foundation. Be my advocate, be my guide, love me for who I am, and we’ll see how far I can go.
10. I am a child. My autism is part of who I am, not all of who I am. Are you just one thing, or are you a person with thoughts, feelings, preferences, ideas, talents, and dreams? Are you fat (overweight), myopic (wear glasses) or klutzy (uncoordinated)? Those may be things that I see first when I meet you, but you’re more than just that, aren’t you?
As an adult, you have control over how you define yourself. If you want to single out one characteristic, you can make that known. As a child, I am still unfolding. Neither you nor I yet know what I may be capable of. If you think of me as just one thing, you run the danger of setting up an expectation that may be too low. And if I get a sense that you don’t think I “can do it,” my natural response will be, why try?
9. My senses are out of sync.This means that ordinary sights, sounds, smells, tastes, and touches that you may not even notice can be downright painful for me. My environment often feels hostile. I may appear withdrawn or belligerent or mean to you, but I’m just trying to defend myself. Here’s why a simple trip to the grocery store may be agonizing for me.
My hearing may be hyperacute. Dozens of people jabber at once. The loudspeaker booms today’s special. Music blares from the sound system. Registers beep and cough, a coffee grinder chugs. The meat cutter screeches, babies wail, carts creak, the fluorescent lighting hums. My brain can’t filter all the input and I’m in overload!
My sense of smell may be highly sensitive. The fish at the meat counter isn’t quite fresh, the guy standing next to us hasn’t showered today, the deli is handing out sausage samples, the baby in line ahead of us has a poopy diaper, they’re mopping up pickles on aisle three with ammonia. I feel like throwing up.
And there’s so much hitting my eyes! The fluorescent light is not only too bright, it flickers. The space seems to be moving; the pulsating light bounces off everything and distorts what I am seeing. There are too many items for me to be able to focus (my brain may compensate with tunnel vision), swirling fans on the ceiling, so many bodies in constant motion. All this affects how I feel just standing there, and now I can’t even tell where my body is in space.
8. Distinguish between won’t (I choose not to) and can’t (I am not able to).It isn’t that I don’t listen to instructions. It’s that I can’t understand you. When you call to me from across the room, I hear, Jordan.” Instead, come over to me, get my attention, and speak in plain words: “Jordan, put your book in your desk. It’s time to go to lunch.” This tells me what you want me to do and what is going to happen next. Now it’s much easier for me to comply.
7. I’m a concrete thinker. I interpret language literally.You confuse me by saying, “Hold your horses, cowboy!” when what you mean is, “Stop running.” Don’t tell me something is “a piece of cake” when there’s no dessert in sight and what you mean is, “This will be easy for you to do.” When you say, “It’s pouring cats and dogs,” I see pets coming out of a pitcher. Tell me, “It’s raining hard.”
Idioms, puns, nuances, inferences, metaphors, allusions, and sarcasm are lost on me.
6. Listen to all the ways I’m trying to communicate.It’s hard for me to tell you what I need when I don’t have a way to describe my feelings. I may be hungry, frustrated, frightened, or confused but right now I can’t find those words. Be alert for body language, withdrawal, agitation or other signs that tell you something is wrong. They’re there.
Or, you may hear me compensate for not having all the words I need by sounding like a little professor or movie star, rattling off words or whole scripts well beyond my developmental age. I’ve memorized these messages from the world around me because I know I am expected to speak when spoken to. They may come from books, television, or the speech of other people. Grown-ups call it echolalia. I may not understand the context or the terminology I’m using. I just know that it gets me off the hook for coming up with a reply.
5. Picture this! I’m visually oriented.Show me how to do something rather than just telling me. And be prepared to show me many times. Lots of patient practice helps me learn.
Visual supports help me move through my day. They relieve me of the stress of having to remember what comes next, make for smooth transition between activities, and help me manage my time and meet your expectations.
I need to see something to learn it, because spoken words are like steam to me; they evaporate in an instant, before I have a chance to make sense of them. I don’t have instant-processing skills. Instructions and information presented to me visually can stay in front of me for as long as I need, and will be just the same when I come back to them later. Without this, I live the constant frustration of knowing that I’m missing big blocks of information and expectations, and am helpless to do anything about it.
4. Focus and build on what I can do rather than what I can’t do. Like any person, I can’t learn in an environment where I’m constantly made to feel that I’m not good enough and that I need fixing. I avoid trying anything new when I’m sure all I’ll get is criticism, no matter how “constructive” you think you’re being. Look for my strengths and you will find them. There is more than one right way to do most things.
3. Help me with social interactions.It may look like I don’t want to play with the other kids on the playground, but it may be that I simply do not know how to start a conversation or join their play. Teach me how to play with others. Encourage other children to invite me to play along. I might be delighted to be included.
I do best in structured play activities that have a clear beginning and end. I don’t know how to read facial expressions, body language, or the emotions of others. Coach me. If I laugh when Emily falls off the slide, it’s not that I think it’s funny. It’s that I don’t know what to say. Talk to me about Emily’s feelings and teach me to ask, “Are you okay?”
2. Identify what triggers my meltdowns. Meltdowns and blow-ups are more horrid for me than they are for you. They occur because one or more of my senses has gone into overload, or because I’ve been pushed past the limit of my social abilities. If you can figure out why my meltdowns occur, they can be prevented. Keep a log noting times, settings, people, and activities. A pattern may emerge.
Remember that everything I do is a form of communication. It tells you, when my words cannot, how I’m reacting to what is happening around me. My behavior may have a physical cause. Food allergies and sensitivities sleep problems and gastrointestinal problems can all affect my behavior. Look for signs, because I may not be able to tell you about these things.
1. Love me unconditionally.Throw away thoughts like, “If you would just—” and “Why can’t you—?” You didn’t fulfill every expectation your parents had for you and you wouldn’t like being constantly reminded of it. I didn’t choose to have autism. Remember that it’s happening to me, not you. Without your support, my chances of growing up to be successful and independent are slim. With your support and guidance, the possibilities are broader than you might think.
Three words we both need to live by: Patience. Patience. Patience.
View my autism as a different ability rather than a disability. Look past what you may see as limitations and see my strengths. I may not be good at eye contact or conversation, but have you noticed that I don’t lie, cheat at games, or pass judgment on other people?
I rely on you. All that I might become won’t happen without you as my foundation. Be my advocate, be my guide, love me for who I am, and we’ll see how far I can go.
|
|
|
Myths Related to Autism
1. Myth: People with autism don’t want friends.
Truth: If someone in your class has autism, they probably struggle with social skills, which may make it difficult to interact with peers. They might seem shy or unfriendly, but that’s just because he or she is unable communicate their desire for relationships the same way you do.
2. Myth: People with autism can’t feel or express any emotion—happy or sad.
Truth: Autism doesn’t make an individual unable to feel the emotions you feel, it just makes the person communicate emotions (and perceive your expressions) in different ways.
3. Myth: People with autism can’t understand the emotions of others.
Truth: Autism often affects an individual’s ability to understand unspoken interpersonal communication, so someone with autism might not detect sadness based solely on one’s body language or sarcasm in one’s tone of voice. But, when emotions are communicated more directly, people with autism are much more likely to feel empathy and compassion for others.
4. Myth: People with autism are intellectually disabled.
Truth: Often times, autism brings with it just as many exceptional abilities as limitations. Many people with autism have normal to high IQs and some may excel at math, music or another pursuit.
5. People with autism are just like Dustin Hoffman’s character in Rain Man.
Truth: Autism is a spectrum disorder, meaning its characteristics vary significantly from person to person. Knowing one person with autism means just that—knowing one person with autism. His or her capabilities and limitations are no indication of the capabilities and limitations of another person with autism.
6. Myth: People who display qualities that may be typical of a person with autism are just odd and will grow out of it.
Truth: Autism stems from biological conditions that affect brain development and, for many individuals, is a lifelong condition.
7. Myth: People with autism will have autism forever.
Truth: Recent research has shown that children with autism can make enough improvement after intensive early intervention to “test out” of the autism diagnosis. This is more evidence for the importance of addressing autism when the first signs appear.
8. Myth: Autism is just a brain disorder.
Truth: Research has shown that many people with autism also have gastro-intestinal disorders, food sensitivities, and many allergies.
9. Myth: Autism is caused by bad parenting.
Truth: In the 1950s, a theory called the “refrigerator mother hypothesis” arose suggesting that autism was caused by mothers who lacked emotional warmth. This has long been disproved.
10. Myth: The prevalence of autism has been steadily increasing for the last 40 years.
Truth: The rate of autism has increased by 600% in the last 20 years. In 1975, an estimated 1 in 1,500 had autism. In 2009, an estimated 1 in 110 had an autism spectrum disorder.
11. Myth: Therapies for people with autism are covered by insurance.
Truth: Most insurance companies exclude autism from the coverage plan and only half of the 50 states currently require coverage for treatments of autism spectrum disorders.
1. Myth: People with autism don’t want friends.
Truth: If someone in your class has autism, they probably struggle with social skills, which may make it difficult to interact with peers. They might seem shy or unfriendly, but that’s just because he or she is unable communicate their desire for relationships the same way you do.
2. Myth: People with autism can’t feel or express any emotion—happy or sad.
Truth: Autism doesn’t make an individual unable to feel the emotions you feel, it just makes the person communicate emotions (and perceive your expressions) in different ways.
3. Myth: People with autism can’t understand the emotions of others.
Truth: Autism often affects an individual’s ability to understand unspoken interpersonal communication, so someone with autism might not detect sadness based solely on one’s body language or sarcasm in one’s tone of voice. But, when emotions are communicated more directly, people with autism are much more likely to feel empathy and compassion for others.
4. Myth: People with autism are intellectually disabled.
Truth: Often times, autism brings with it just as many exceptional abilities as limitations. Many people with autism have normal to high IQs and some may excel at math, music or another pursuit.
5. People with autism are just like Dustin Hoffman’s character in Rain Man.
Truth: Autism is a spectrum disorder, meaning its characteristics vary significantly from person to person. Knowing one person with autism means just that—knowing one person with autism. His or her capabilities and limitations are no indication of the capabilities and limitations of another person with autism.
6. Myth: People who display qualities that may be typical of a person with autism are just odd and will grow out of it.
Truth: Autism stems from biological conditions that affect brain development and, for many individuals, is a lifelong condition.
7. Myth: People with autism will have autism forever.
Truth: Recent research has shown that children with autism can make enough improvement after intensive early intervention to “test out” of the autism diagnosis. This is more evidence for the importance of addressing autism when the first signs appear.
8. Myth: Autism is just a brain disorder.
Truth: Research has shown that many people with autism also have gastro-intestinal disorders, food sensitivities, and many allergies.
9. Myth: Autism is caused by bad parenting.
Truth: In the 1950s, a theory called the “refrigerator mother hypothesis” arose suggesting that autism was caused by mothers who lacked emotional warmth. This has long been disproved.
10. Myth: The prevalence of autism has been steadily increasing for the last 40 years.
Truth: The rate of autism has increased by 600% in the last 20 years. In 1975, an estimated 1 in 1,500 had autism. In 2009, an estimated 1 in 110 had an autism spectrum disorder.
11. Myth: Therapies for people with autism are covered by insurance.
Truth: Most insurance companies exclude autism from the coverage plan and only half of the 50 states currently require coverage for treatments of autism spectrum disorders.
|
|
|
Resources For Educators
|
Academic modifications
Students with ASD will more than likely need to have some form of academic modification while in their general education class, regardless of intellectual ability.8 Issues with fine-motor deficits (e.g., grasping a pencil to write) and motivation (e.g., attending to heavy workloads in some subjects) are among some of the areas that may require modifications.9 There are numerous ways for teachers to modify activities and materials to meet the needs of students with ASD. In many cases, modifications that are appropriate for students with learning disabilities can also be useful for students with ASD. For example, adjusting the number of items that the student must complete can be helpful, such as requiring the student to complete only the even numbers on a math activity. This helps maintain the student’s attention without overwhelming her, while giving the teacher enough data to determine if the student has mastered the skill. The time allowed for completing assignments can also be adjusted, giving extra time if needed to accommodate fine-motor deficits. Teachers can also increase the level of support that the student with ASD receives during a lesson, such as peer or paraprofessional support during math instruction. Another useful modification is varying the response modes for the student. For example, a student who struggles with writing may be allowed to type responses or verbally answer questions. Modifying the student’s environment so that he or she can learn successfully is another consideration. The location of the student’s desk and materials is important. The desk should be as close to the teacher as possible and should face the front of the room. A quiet zone in the classroom is helpful when the student becomes “overloaded” with stimuli. Sensory materials, like a bean bag or stress ball, and sensory-blocking materials, like earplugs or earphones, can increase the student’s level of engagement by occupying or isolating a particular sense. Some students with ASD do not tolerate noise very well, so having the option for the student to request using the quiet zone with earplugs may calm the student if he’s feeling overloaded. |
Communication strategies
The first and most critical element of developing strategies to support communication in a student with ASD is teacher knowledge. Teachers must begin with an awareness of the student’s communication abilities. It may be helpful to remember that every behavior is an attempt at communication. If the student has no functional language or is nonverbal, it is imperative that teachers use nonverbal communication — such as pairing gestures with speech, or pointing to the science textbook in the student’s desk while asking students to get out their science textbooks. Teachers should try to determine communicative attempts displayed by the student’s behavior. For example, if a nonverbal student with ASD screams halfway through literacy instruction and the teacher allows the student to stop the activity, that student has successfully “escaped” the undesired activity by screaming. An alternative scenario might involve the teacher instructing the student to communicate needing a break by handing the teacher a picture symbol for “break” — however, the teacher should always have the student return to the activity after taking a break to ensure that the student does not use “break” to escape the activity. Reinforcing the correct behavior (asking for “break” appropriately) and ignoring inappropriate behavior (screaming) can be a successful strategy. When it’s difficult to determine the function of a student’s behavior, a teacher may benefit from using a behavior plan that indicates the use of an A-B-C form. An A-B-C form provides a format for teachers to write down the Antecedent — what happened directly before the behavior, the Behavior — what the student specifically did, and the Consequence — what happened directly after the behavior that maintained the behavior. 
|
Socialization strategies
Teaching social skills to students with ASD is extremely important, and is beneficial not only for the student but for classmates as well. Classmates have been known to “benefit from their experiences with students with ASD, developing a compassion for and an understanding of children with special needs. Their self-esteem is boosted by the positive role they take in helping a friend with autism learn.”10 Teachers should always supervise social interactions, and can offer valuable support by providing specific social rules and reinforcing positive social interactions. This can be done by posting specific social rules easily visible and understandable by all students, and reviewed periodically with the class. Teachers should recognize that a student with ASD may want to interact, but may not know how. Helping the student change topics of the conversation when necessary, rehearsing strategies for social interactions, and using classmates as peer models (e.g., video modeling of a desired social skill) are notable strategies, as well as providing “scripts” of what the student should do in particular social situations. |